JDO Vol. 65
Editorial
“There is nothing like writing to force you think and get your thoughts straight.” — Warren Buffet
Dr. Chris H. Chang
This quote above encapsulates exactly what writing means to me. During the last 30 years of my orthodontic journey, I have always considered writing to be the one skill that has enabled me to meticulously organise my thoughts. It will therefore come as no surprise to you that case report writing is a fundamental and crucial part of our clinic’s residency training…
{kind=link}
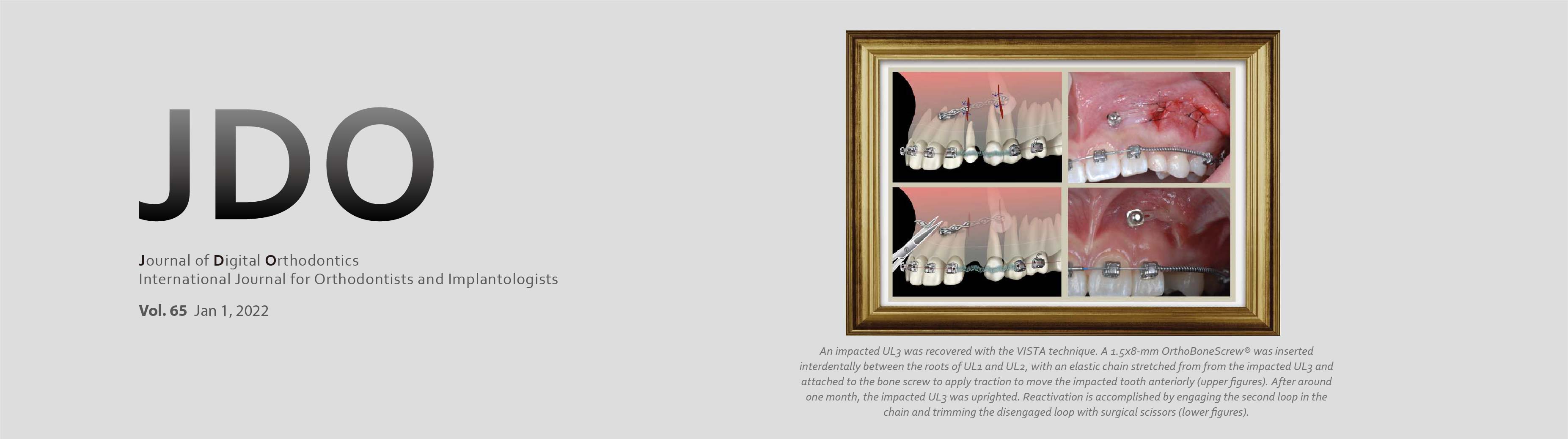
Class II Malocclusion with Impacted and Transposed Canines Treated with Modified Vertical Incision Subperiosteal Tunnel Access (VISTA) and Bone Screws
Joy Cheng, Chris H. Chang, W. Eugene Roberts
Abstract
Introduction: A 11yr-8mo-old female presented with a chief complaint of unerupted bimaxillary right canines.
Diagnosis: The patient had a right end-on Class II and left full-cusp Class II dental malocclusion with an overjet of 8mm. A 100% impinging deep bite was also noted. This severe malocclusion was further complicated by an incompletely transposed and impacted maxillary right canine and a completely transposed and impacted mandibular right canine. The discrepancy index (DI) was 59.
Etiology: The cause of the severe impaction was a deviated path of eruption that may be related to over-retained primary canines.
Treatment: A right-sided infra-zygomatic crest (IZC) bone screw and a right-sided buccal shelf (BS) bone screw were used as anchorage for a modified vertical incision subperiosteal tunnel access (VISTA) submucosal procedure to retract unerupted bimaxillary right canines to their correct sagittal relationships, respectively. Bilateral IZC bone screws, Class II elastics, combined with anterior and posterior bite turbos (BTs) were used to correct the Class II malocclusion, excessive overjet, and deep bite.
Outcome: After 35 months of active treatment, this difficult malocclusion, with a Discrepancy Index of 59 points, achieved a Cast-Radiograph Evaluation score of 26 points and a Pink and White esthetic score of 4 points. The patient was very pleased with the treatment outcome. Final records were collected at the 1.5-year recall appointment. (J Digit Orthod 2022;65:4-24, reprinted with permission from Int J Orthod 2021;32(2):7-17)
Key words: Impaction, impacted and transposed maxillary canine, impacted and transposed mandibular canine, incompletely transposed impaction, completely transposed impaction, modified vertical incision subperiosteal tunnel access, VISTA, bone screw, closed eruption technique
Download Article
Managing a Labially-Impacted Canine with VISTA, Connective Tissue Graft, IZC Screws, and a 3D Lever Arm
Jeff Y. Lee, Chris H. Chang, W. Eugene Roberts
Abstract
History: A 13year-2month-old male presented with chief complaints (CC) of an unesthetic smile and diastema.
Diagnosis: The upper right deciduous canine (URc) was retained, and the UR3 was labially impacted. An oblique direction of canine eruption wedged the impaction between the keratinized mucosa and the adjacent incisor. His lower facial height was within normal limits (WNL) (%FH: Na-ANS-Gn 53%), but the profile was more convex than normal (Convexity: G-Sn-Pg’ 20˚). Bilateral molars were in full-cusp Class II malocclusion. Mandibular retrusion (SNB 76˚) and a normal mandibular angle (SN-MP 33˚) were noted. Bilateral incisors were prominent (U1 to NA 9mm, U1 to SN 118˚, L1 to NB 6.5mm, L1 to MP 99˚). The Discrepancy Index (DI) was 37.
Etiology: The severely impacted UR3 was apparently due to a deviated path of eruption, which may be related to improper development of the tooth, and/or limited space in the arch.
Treatment: Following extraction of the URc, all teeth except the UR2 were bonded with a Damon Q® passive self-ligating (PSL) bracket system. Vertical incision subperiosteal tunnel access (VISTA) technique was performed to produce a submucosal space for retracting and extruding the impacted UR3. A button was bonded on the UR3, and a power chain was attached. The elastomer chain exited the mucosa through a more distal incision, and traction was applied with a custom lever arm, anchored by an OrthoBoneScrew® (OBS) inserted into the right infrazygomatic crest (IZC). The impaction was retracted into a normal position between the UR2 and UR4. Once the UR3 was extruded and approached the occlusal plane, the UR2 was bonded. The VISTA technique can be used in combination with a connective tissue graft (CTG) to treat UR3 gingival recession defects. A slow traction procedure, with regular periodontal maintenance, was performed to avoid a premature perforation of the labial alveolar plate. Both arches were detailed and finished.
Outcomes: Facial esthetics was improved. After 33 months of active treatment, the UR3 was well aligned. The supporting labial gingiva matured and keratinized without any additional root resorption. Final alignment and dental esthetics were excellent, as evidenced by an ABO Cast-Radiograph Evaluation (CRE) score of 24, and an IBOI Pink and White esthetic score of 8.
Conclusions: The VISTA approach with an OBS-anchored 3D lever arm for submucosal retraction of maxillary canine impactions is an ideal procedure for the critical esthetic zone. Differential soft and hard tissue biomechanics protect an unrestrained lateral incisor while the impacted canine is being recovered. (J Digital Orthod 2022;65:30-47)
Key words: Tooth movement, eruptive force, differential biomechanics, impacted maxillary canine, vertical incision subperiosteal tunnel access (VISTA)
Download Article
CLINICAL TIPS:
Management of Maxillary Impactions: Four Surgical Techniques
Joshua Lin, Chris H. Chang, W. Eugene Roberts
(J Digit Orthod 2022;65:56-82)
A. Uncovering via Excision (E), the Open-Window Technique
Kokich et al. suggested that a palatal impaction will spontaneously emerge after obstructing soft and hard tissue are removed along the desired path of eruption. The open window via excision (E) method is optimal for most palatal impactions. In addition to excising overlying soft tissue, bone obstructing eruption must be removed down to the cementoenamel junction (CEJ). In effect, the entire clinical crown must be exposed in the desired path of eruption. Post-operative (post-op) periodontal dressing is required for deep impactions to prevent healing tissue from covering the exposed crown and obstructing eruption. Adequately exposed teeth usually erupt into the oral cavity spontaneously. Since the entire palate is covered by attached mucosa, there is little problem in achieving an adequate keratinized gingiva to support a tooth recovered from the palate.B. Apically Positioned Flap (APF)
An APF is a common periodontal surgery designed to decrease pocket depth, maintain an adequate zone of keratinized tissue, and lengthen the clinical crown for a prosthesis. A gingivectomy to uncover an impaction decreases the width of keratinized tissue, but an APF increases keratinized gingiva via a secondary healing process. Kokich recommends an APF to uncover an impaction if it is at, or apical to, the MGJ.C. Closed Eruption (CE)
The CE technique is preferred for most labially impacted teeth, particularly if they are located apical to the mucogingival junction (MGJ). The APF technique is difficult or impossible to use for most very high impactions.Some clinicians believe that CE with orthodontic traction simulates the natural tooth eruption process to produce the most ideal periodontal results. The CE technique is the most predictable for high impactions particularly on the labial surface.
D. Modified Vestibular Incision Subperiosteal Tunnel Access (VISTA)
Access to the surgical site is obtained by vestibular incision subperiosteal tunnel access (VISTA). Zadeh developed VISTA as a novel, minimally invasive approach for managing isolated recession and multiple contiguous defects in the maxillary anterior region. VISTA offers the opportunity to coronally reposition the margins on teeth with gingival recession and/or osseous defects. It is a flapless surgical technique with minimal soft tissue trauma that provides good surgical access and is much more comfortable for the patient. The VISTA technique can be applied with connective tissue and particle bone grafts when managing gingival recession with osseous defects. Since no flap is reflected, tension across the wound is decreased, which facilitates closure with direct loop interrupted sutures.Chang et al. modified the VISTA technique for managing maxillary anterior impactions with or without tooth transposition. The modified VISTA approach provides a much more comfortable experience for patients with a facilitated wound healing process that is particularly well suited for surgical management of labial impactions in the esthetic zone. This method is a minimally invasive approach for producing optimal dental esthetics.
A Biographical Portrait of Edward Hartley Angle, the First Specialist in Orthodontics, Part 3
Sheldon Peck
Abstract
Reprinted from News & Trends in Orthodontics 2009;16:21-23, originally reprinted with permission from Angle Orthod 2009;79:1034-1036. Copyright 2009). (J Digital Orthod 2022;65:88-93)
Taiwanese Lifestyle Through the Eyes of CC
Chapter 4. Outdoor Free-Flight Training
A bird in hand is a certainty. But a bird in the bush may sing. — Bret Harte
When shown the videos of the Changs’ cockatiel Juno and monk parakeet (also known as a Quaker parrot) Bagel in the neighborhood reserve, sometimes flying freely and sometimes leisurely perching on Dr. Chang’s shoulders for a stroll, the bird shop owner from where these feathered children were purchased was simply lost for words. During the 40 odd years that he has been running his business, never had he imagined that these birds would be able to develop such a bond with their keeper, especially when taken outdoors.
Free flight outdoors for pet birds is as much of a training course for humans as it is for birds; the safety of the birds must be ensured and potential heartbreak for the owners can be prevented…